Fetal Alcohol Syndrome Face: Signs and Features Explained
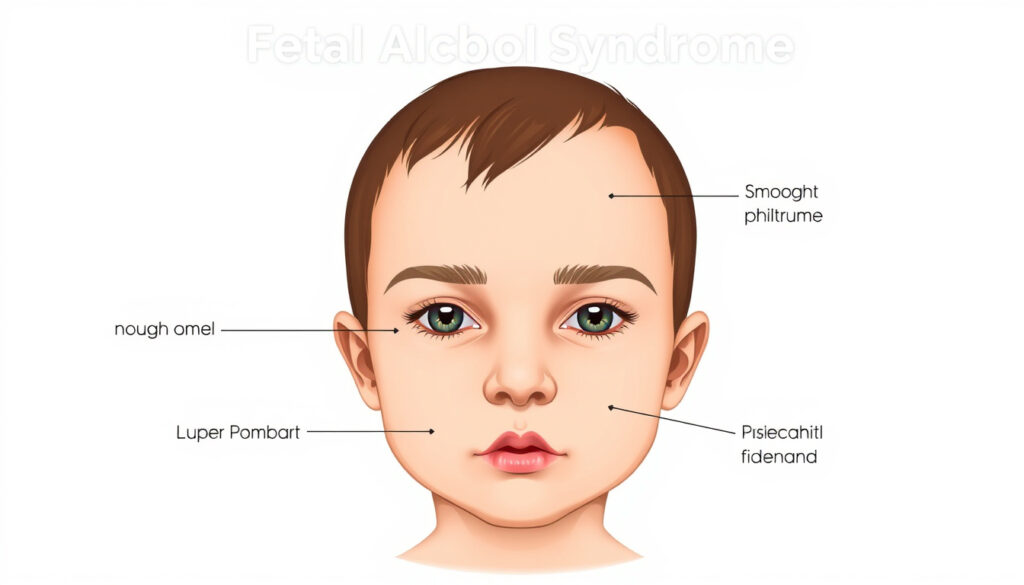
Most people have never heard of a philtrum, yet it’s one of the first things a clinician looks for when assessing fetal alcohol syndrome. The three distinctive facial features that signal this condition—smooth philtrum, thin upper lip, and short palpebral fissures—are specific enough that their combination is called pathognomonic, meaning it points distinctly to prenatal alcohol exposure. According to the CDC, these markers form the cornerstone of clinical identification, and they’re measurable enough to score on standardized scales.
Key Facial Features: Short palpebral fissures, smooth philtrum, thin upper lip · Cause: Prenatal alcohol exposure · Affected Structures: Brain, spinal cord, face · Diagnostic Markers: 3 dysmorphic facial features · Prevalence Note: No safe alcohol amount during pregnancy
Quick snapshot
- Smooth philtrum, thin upper lip, short palpebral fissures form a pathognomonic triad specific to prenatal alcohol exposure (FASD Hub Australia)
- The exact alcohol threshold that produces FASD facial features remains uncertain (FASD Hub Australia)
- AAFP published detailed FAS facial criteria in 2005; PMC study on objective measures appeared in 2013 (AAFP)
- Objective evaluation tools using philtrum luminosity and lip circularity are advancing diagnostic precision (FASD United)
The table below summarizes the key diagnostic facial markers used in FAS clinical assessment.
| Defining Facial Traits | Short palpebral fissures, smooth philtrum, thin upper lip |
|---|---|
| Primary Cause | Alcohol use during pregnancy |
| Key Dysmorphology | Underdeveloped medial nasal processes |
| Common in FAS | Small eyes, flat nasal bridge |
| Palpebral Fissure Threshold | ≤10th percentile or 2+ SD below mean |
| Astley Scale Scores | 4 or 5 indicates abnormality |
| Minimum for Partial FAS | 2 of 3 facial features present |
What are the facial signs of fetal alcohol syndrome?
The diagnostic triad for fetal alcohol syndrome consists of three measurable facial features: a smooth philtrum, a thin upper lip, and shortened palpebral fissures. The philtrum is the vertical groove between the nose and upper lip—normally it has a defined ridge, but in FAS it appears flat or smooth. The University of Washington defines smooth philtrum as a vertical groove that is absent or diminished, and short palpebral fissures as a distance 2 or more standard deviations below the mean.
In newborns and children
In infants and young children, the three sentinel facial features may be visible even before developmental delays become apparent. The American Academy of Pediatrics notes distinctive dysmorphic features: small palpebral fissures, smooth philtrum, and thin upper lip or vermillion border—with all three required for a formal FAS diagnosis (American Academy of Pediatrics). Short palpebral fissures appear as narrowed eye openings, and the upper lip lacks the full, defined border seen in typical facial structure. The flat nasal bridge common in FAS further contributes to the recognizable facial profile.
In adults
Facial features associated with FAS persist into adulthood, though measurement standards apply the same thresholds. Research published in PMC notes that the classic facial characteristics—shortened palpebral fissures, smooth philtrum, and thin upper vermillion—remain diagnostic markers regardless of age (PMC-NIH). While facial features may become less pronounced over time, clinical assessment still applies percentile and standard deviation measurements to confirm presence of the sentinel features.
What are 5 signs and symptoms of FASDs?
Fetal alcohol spectrum disorders extend beyond facial features to affect multiple body systems. The CDC diagnostic criteria for FAS require three specific facial findings—smooth philtrum, thin vermilion border of upper lip, short palpebral fissures—but the condition also involves growth deficiencies and central nervous system abnormalities (AAFP). These facial abnormalities alone are insufficient for diagnosis, which is why clinicians assess a broader constellation of signs.
Physical symptoms
- Growth deficiencies including low birth weight and slowed growth velocity
- Facial dysmorphology: the three sentinel features plus flat midface and low nasal bridge
- Small head circumference (microcephaly)
- Damage to brain and spinal cord structures
Brain and central nervous system issues
- Structural brain abnormalities affecting cognitive function
- Central nervous system problems including motor skill deficits
- Behavioral and learning difficulties
- Executive function impairment
SHAAP emphasizes that FASD is not solely about the face—CNS and growth deficits are equally important diagnostic components that distinguish the full spectrum of effects from partial presentations.
How to tell someone has fetal alcohol syndrome?
Diagnosis of fetal alcohol syndrome requires a combination of confirmed facial dysmorphology and documented prenatal alcohol exposure, though the CDC notes that exposure confirmation is not always required for FASD diagnosis. The FASD Hub explains that while these facial features may occur independently as normal variations in the general population, when seen in combination, they are pathognomonic of and highly specific to prenatal alcohol exposure. This means the triad alone carries strong diagnostic weight even without other supporting evidence.
Facial feature checklist
- Smooth philtrum: Absent or diminished vertical groove between nose and upper lip, scored 4 or 5 on the Astley scale
- Thin upper lip: Narrow vermillion border, scored 4 or 5 on the Astley scale
- Short palpebral fissures: Eye opening distance at or below the 10th percentile
- Flat nasal bridge and small eye openings as supporting features
Behavioral indicators
- Underdeveloped medial nasal processes lead to characteristic facial profile
- CNS abnormalities may manifest as attention or learning difficulties
- Growth deficiencies documented across developmental trajectory
The AAP warns of overlap between FAS dysmorphic facial features and those seen in other genetic syndromes, making differential diagnosis essential. Clinical presentation alone cannot confirm FASD—comprehensive evaluation rules out other causes.
What are the personality traits of someone with FASD?
Behavioral and personality characteristics in individuals with FASD reflect underlying brain and central nervous system involvement. AACAP notes that abnormal facial features in FASD include small eye openings, smooth philtrum, and thin upper lip, but these physical markers often accompany a distinct behavioral profile that clinicians recognize as part of the broader presentation. While not all individuals with FASD share identical behavioral traits, certain patterns appear with enough frequency to warrant clinical attention.
In children
- Difficulty with executive function and impulse control
- Challenges with attention and concentration
- Learning difficulties disproportionate to intellectual capacity
- Social and interpersonal skill deficits
Long-term behaviors
- Ongoing difficulties with organizational skills and planning
- Increased risk of mental health conditions including anxiety and depression
- Challenges with adaptive functioning and daily living skills
- Potential for secondary conditions without appropriate support
How much alcohol can cause FASD?
The relationship between alcohol exposure and FASD presents one of the clearest messages in preventive medicine: there is no established safe amount of alcohol during pregnancy. The CDC, AAP, and virtually every major health authority concur that any prenatal alcohol exposure carries risk, and the precise threshold that produces the characteristic facial features remains scientifically undefined. The FASD Hub acknowledges this directly when noting that the exact alcohol threshold for FASD onset is unclear.
Risk thresholds
No research has established a minimum dose below which facial dysmorphology will not occur. AAFP reports that FAS diagnosis requires confirmed maternal alcohol throughout gestation plus facial features, but this reflects clinical criteria rather than a biological threshold. Individual susceptibility varies based on genetic factors, timing of exposure during pregnancy, and other variables that science has not fully characterized.
No safe level
The CDC emphasizes that prenatal alcohol exposure is the direct cause of FAS facial features, and guidance consistently states that no safe amount exists. The absence of a defined threshold does not imply that light or occasional drinking is safe—it means the risk window is open throughout pregnancy and individual responses cannot be predicted. This uncertainty is precisely why public health messaging emphasizes complete abstinence during pregnancy.
The absence of a defined safe threshold means that any alcohol consumption during pregnancy carries potential risk for facial dysmorphology. Unlike some teratogens with known minimum doses, alcohol lacks a clear safety boundary for FASD prevention.
Confirmed facts
- Facial features from prenatal alcohol: smooth philtrum, thin lip, short fissures
- CDC diagnostic criteria for FAS require three specific facial findings
- Astley scale scores 4 or 5 indicate abnormality
- Short palpebral fissure defined as ≤10th percentile
- ≥2 of 3 facial features diagnostic for partial FAS
What’s unclear
- Exact alcohol threshold for FASD onset
- Individual susceptibility variation factors
- Precise timing during pregnancy that produces facial features
Although these facial features may also occur independently as normal variations in the general population (unrelated to prenatal alcohol exposure), when seen in combination, these facial features are pathognomonic of and highly specific to prenatal alcohol exposure.
— FASD Hub Australia (Australian FASD Resource)
Classic facial characteristics of fetal alcohol syndrome (FAS) are shortened palpebral fissures, smooth philtrum, and thin upper vermillion.
— PMC-NIH Authors (Peer-reviewed Research)
Fetal Alcohol Spectrum Disorder: It’s not all about the face!
— SHAAP (Scottish Health Action on Alcohol Problems)
For healthcare providers, the clinical picture of fetal alcohol syndrome represents one of the most specific diagnosis scenarios in developmental disorders—when the three sentinel facial features appear together, the pathognomonic link to prenatal alcohol exposure is established. Yet this diagnostic clarity coexists with persistent uncertainty: no amount of alcohol has been proven safe, no threshold definitively identifies who will develop facial dysmorphology, and the behavioral manifestations of FASD can evolve over a lifetime without intervention. For families seeking diagnosis, for clinicians refining their assessment skills, and for public health officials crafting prevention messaging, the challenge remains translating what we know with certainty into actionable guidance that prevents harm before it occurs.
Related reading: alcohol health risks
cdc.gov, depts.washington.edu, shaap.org.uk, specialolympicsarizona.org
Key indicators like smooth philtrum, thin upper lip, and short palpebral fissures serve as primary biomarkers, as explored in Swedish guide to facial traits for precise clinical identification.
Frequently asked questions
Does FASD get worse with age?
The facial features of FASD persist throughout life, but their diagnostic significance may shift as individuals age and natural facial changes occur. However, the underlying brain and central nervous system impacts do not resolve, and without appropriate support, secondary conditions such as mental health challenges, academic difficulties, and adaptive functioning problems often become more apparent over time. Early intervention can mitigate some long-term outcomes, but the neurological basis of FASD does not change with age.
Is FAS a type of autism?
FAS is not classified as a type of autism spectrum disorder. Both conditions can involve social and behavioral challenges, and they may co-occur in some individuals, but they are distinct diagnostic categories with different underlying causes. FAS results from prenatal alcohol exposure while autism has neurodevelopmental origins not linked to alcohol exposure. Some symptoms may overlap, which is why differential diagnosis by qualified clinicians is essential.
Is FAS part of autism?
FAS is not considered part of autism spectrum disorder. These are separate conditions with distinct etiologies. FAS falls under the fetal alcohol spectrum disorders category and results from confirmed or suspected prenatal alcohol exposure. While individuals with FASD may share some behavioral characteristics with autism, such as social difficulties or repetitive behaviors, the diagnostic criteria, causes, and recommended interventions differ significantly.
Can fetal alcohol syndrome lead to autism?
FAS itself does not cause autism, but research indicates that individuals with FASD may have higher rates of autism spectrum disorder than the general population. The two conditions can co-occur because both involve brain development impacts, though they arise from different mechanisms. Prenatal alcohol exposure causes the structural and functional differences characteristic of FASD, while autism has distinct developmental origins. Co-occurring FASD and autism require integrated treatment approaches addressing both conditions.
What mental illness is associated with fetal alcohol syndrome?
FASD is associated with increased risk of several mental health conditions including anxiety disorders, depression, attention deficit hyperactivity disorder (ADHD), and substance use disorders. The central nervous system damage caused by prenatal alcohol exposure affects emotional regulation, impulse control, and executive function—all factors contributing to mental health vulnerability. Individuals with FASD benefit from mental health monitoring and intervention as part of comprehensive care.
Meer gerelateerde berichten
 Blackwall Tunnel Charge Times: Schedule, Free Hours & Payments
Blackwall Tunnel Charge Times: Schedule, Free Hours & Payments
 Cristiano Jr: Age, Height, Mother, and Football Stats
Cristiano Jr: Age, Height, Mother, and Football Stats
 John Davidson Tourette: Activist, Documentary, and BAFTA Incident
John Davidson Tourette: Activist, Documentary, and BAFTA Incident
 Yung Chow Fried Rice: Origins, Ingredients & Recipe
Yung Chow Fried Rice: Origins, Ingredients & Recipe
 Carla Connor: A Guide to Her Marriages, Tragedies, and Love Life
Carla Connor: A Guide to Her Marriages, Tragedies, and Love Life
 Co-Codamol Side Effects – Common Symptoms and Serious Risks
Co-Codamol Side Effects – Common Symptoms and Serious Risks
